As of 2024, there were 24 million noncitizen immigrants, including lawfully present and undocumented immigrants, living in the U.S. Noncitizen immigrants, particularly those who are undocumented, face significant barriers to accessing health coverage and care and are significantly more likely than citizens to be uninsured. These higher uninsured rates reflect more limited access to private coverage and eligibility restrictions for federally funded coverage options. Undocumented immigrants are not eligible for federally funded coverage options and lawfully present immigrants face eligibility restrictions for coverage. Under the 2025 reconciliation law there will be increased eligibility restrictions for many lawfully present immigrants for Medicaid and the Children’s Health Insurance Program (CHIP), subsidized Affordable Care Act (ACA) Marketplace coverage, and Medicare coverage.
Some states have taken up options in Medicaid and CHIP to expand coverage for lawfully present immigrants and/or established fully state-funded programs to fill gaps in coverage for immigrants. However, some states have recently made reductions to these programs due to budget pressures. On the other hand, a few states are considering how they can use state funded coverage to fill the gaps in coverage that will result from the reconciliation law eligibility restrictions. This brief provides an overview of state take-up of these options and fully state-funded health coverage programs for immigrants.
As of April 2026, 15 states, including DC, provide fully state-funded coverage for income-eligible children regardless of immigration status; seven states, including DC, provide fully state-funded coverage to some income-eligible adults regardless of status; and most states have taken up options in Medicaid and CHIP to expand coverage to lawfully present immigrant children and pregnant people. Six states, including DC, have recently scaled back their state funded coverage for adults. Two states have plans to expand state-funded coverage to fill gaps in coverage that will be created by the 2025 reconciliation law eligibility restrictions, and several other states have pending legislation to fill gaps.
Looking ahead, states may face increased challenges maintaining state-funded coverage programs, while at the same time there may be growing need for coverage due to new restrictions in federally funded coverage for lawfully present immigrants under the reconciliation law. More limited access to federally funded coverage as well as reductions in state-funded coverage programs will likely lead to increases in uninsured rates for immigrant families contributing to greater challenges accessing care and potentially worse health outcomes over the long-term. These changes could also have negative implications for the U.S. economy and workforce, where immigrant families make significant contributions.
Health Coverage for Immigrants
Lawfully present immigrants may qualify for federally funded coverage but face eligibility restrictions. For example, many must meet a five-year waiting period before qualifying for Medicaid or CHIP even if they meet other eligibility criteria. Lawfully present immigrants can purchase coverage through the ACA Marketplaces and may receive tax credits for this coverage without a waiting period. Lawfully present immigrants have been eligible for Medicare if they have the required work quarters and meet the disability or age requirements. Under the 2025 reconciliation law, eligibility for Medicaid and CHIP, subsidized Marketplace, and Medicare coverage will be limited to immigrants who are lawful permanent residents (LPRs) or green card holders, certain Cuban and Haitian entrants, and people residing in the U.S. as citizens of the Freely Associated (COFA) nations of the Marshall Islands, Micronesia, and Palau. The law also eliminates ACA Marketplace coverage for lawfully present immigrants with incomes less than 100% FPL effective January 1, 2026. States may also continue to cover lawfully residing children and pregnant immigrants under a Medicaid or CHIP option. These changes will result in some groups of lawfully present immigrants losing access to federally funded coverage, including refugees and asylees.
Undocumented immigrants are ineligible to enroll in federally funded coverage, including Medicaid or CHIP, the ACA Marketplaces, or Medicare. Medicaid payments for emergency services reimburse hospitals for emergency care they are obligated to provide to individuals who meet other Medicaid eligibility requirements (such as income), but who do not have an eligible immigration status, including undocumented immigrants as well as some lawfully present immigrants. These payments help cover costs to hospitals for providing emergency care to immigrants who remain ineligible for Medicaid but are not coverage for individuals. Emergency spending accounted for less than one percent of total Medicaid spending between fiscal years 2017 and 2023. The 2025 reconciliation law reduces the federal Medicaid matching rate provided to states for Emergency Medicaid services provided to expansion adults who would otherwise be eligible for Medicaid except for their immigration status to the regular matching rate starting October 1, 2026.
State Take-up of Optional Coverage for Lawfully Present Immigrants
Most states have taken up options in Medicaid and CHIP to expand coverage for lawfully residing children and/or pregnant people. In general, lawfully present immigrants must have a “qualified” immigration status to be eligible for Medicaid or CHIP, and many, including most lawful permanent residents or “green card” holders, must wait five years after obtaining qualified status before they may enroll even if they meet other eligibility requirements. Some immigrants, such as those with Temporary Protected Status, are lawfully present but do not have a qualified status and are not eligible to enroll in Medicaid or CHIP regardless of their length of time in the country. As noted, under the 2025 reconciliation law, eligibility will be further restricted to lawfully present immigrants who are LPRs or green card holders, certain Cuban and Haitan entrants, and people residing in the U.S. under COFA starting October 1, 2026. States can provide coverage to lawfully residing children and pregnant people without a five-year wait under the Immigrant Children’s Health Improvement Act (ICHIA) option. As of April 2026, 38 states, including DC, have taken up this option for children and 32 states, including DC, have elected the option for pregnant people (Figure 1). States may continue to provide this coverage under the 2025 reconciliation law. North Carolina enacted a Medicaid funding bill in April 2026 that codified the 2025 reconciliation law’s immigrant eligibility changes by limiting eligibility to coverage that the state is federally required to provide, starting October 1, 2026. This would eliminate ICHIA coverage as it is optional for states to provide. However, the Governor has called for the state legislature to reinstate this coverage and some state legislators have indicated that the cut was unintentional.
A total of 25 states, including DC, have extended coverage through the CHIP From-Conception-to-End-of-Pregnancy (FCEP) option, which provides prenatal care and pregnancy related benefits to eligible low-income children beginning from conception to end of pregnancy regardless of their parent’s citizenship or immigration status (Figure 2). While other pregnancy-related coverage in Medicaid and CHIP requires 60 days of postpartum coverage, the CHIP FCEP option does not include this coverage. However, some states that took up this option provide postpartum coverage through a CHIP health services initiative or using state-only funding. Eleven of the states that have implemented the FCEP option (California, Colorado, Connecticut, Illinois, Maine, Massachusetts, Minnesota, New York, Oregon, Rhode Island, and Washington) have used state funding or CHIP health services initiatives to extend postpartum coverage to 12 months to align with the Medicaid extension established by the American Rescue Plan Act. Maryland extends coverage for four months postpartum, and Alabama, Texas, Virginia, and DC extend coverage for 60 days postpartum using CHIP health services initiatives.
Fully State-Funded Coverage
Beyond state take-up of options in Medicaid and CHIP for lawfully present immigrants, some states provide fully state-funded coverage to fill gaps in coverage for immigrants. States vary in the eligibility and scope of benefits offered through these coverage programs. These programs extend coverage to lawfully present immigrants who are in the five-year waiting period for Medicaid or CHIP or do not have “qualified status” and are ineligible for federally funded coverage as well as undocumented immigrants. These programs also extend coverage to Deferred Action for Childhood Arrivals (DACA) recipients who are not considered lawfully present for purposes of eligibility for federally funded health coverage programs. While the Biden administration had published regulations to extend Marketplace coverage to DACA recipients, new regulations by the Trump administration and the 2025 reconciliation law excluded them from coverage.
As of April 2026, 15 states, including DC, provide comprehensive state-funded coverage for children regardless of immigration status, with one state (Colorado) planning to scale back coverage due to budget pressures (Figure 3). These states include California, Colorado, Connecticut, Illinois, Maine, Massachusetts, Minnesota, New Jersey, New York, Oregon, Rhode Island, Utah, Vermont, Washington, and DC. Three of these states (Colorado, New Jersey, and Vermont) also provide state-funded coverage to income-eligible pregnant people regardless of immigration status, with Vermont extending this coverage for 12 months postpartum. Colorado plans to implement rollbacks to their state-funded coverage program for children and pregnant people, including capping enrollment and limiting certain benefits, starting January 2027 due to funding constraints.
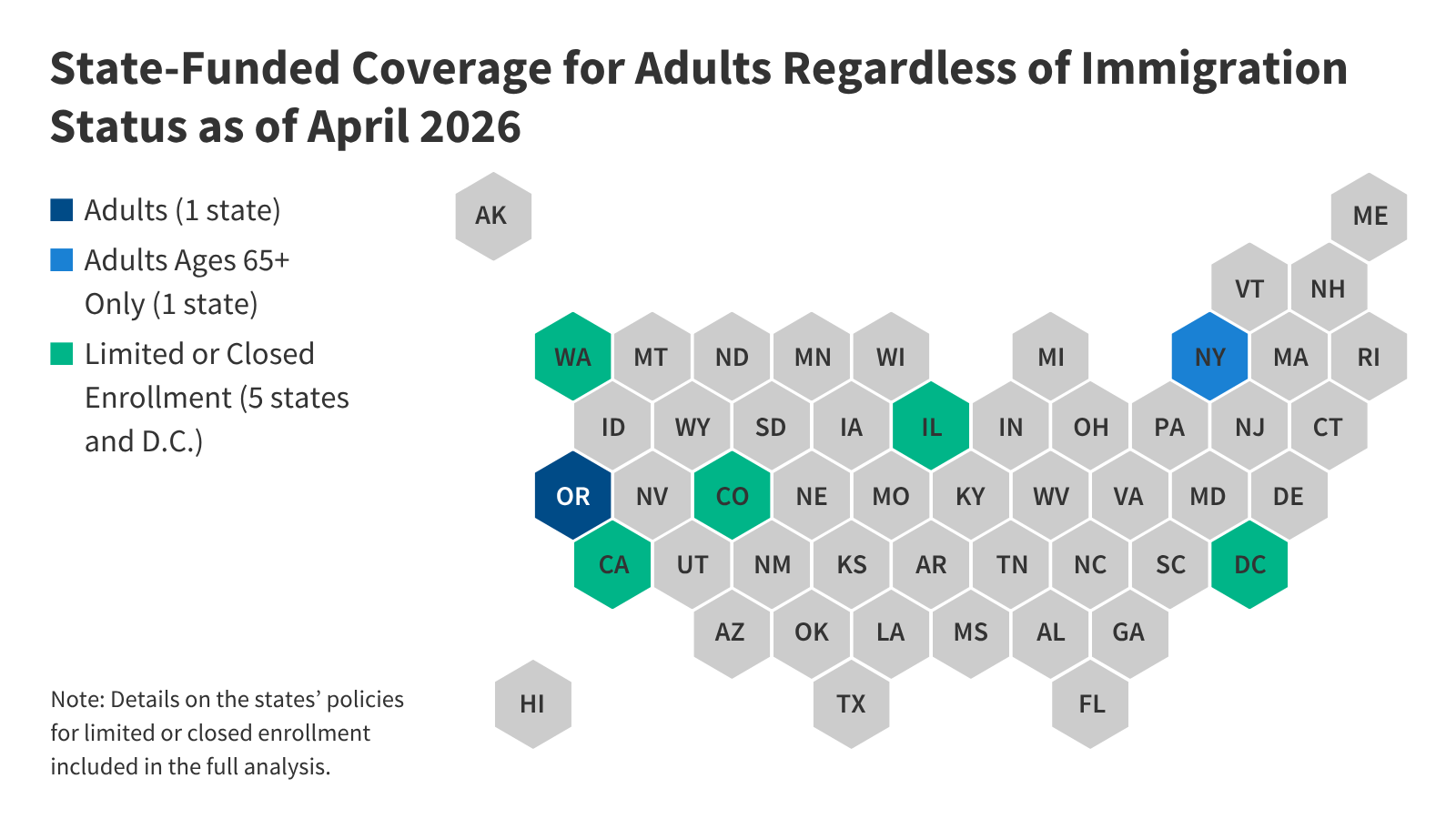
As of April 2026, seven states, including DC, have also expanded fully state-funded coverage to at least some income-eligible adults regardless of immigration status (Figure 4). These states include California, Colorado, DC, Illinois, New York, Oregon, and Washington. In some cases, coverage is limited to certain age groups, and several states have closed new enrollment. Some additional states cover some income-eligible adults who are not otherwise eligible due to immigration status using state-only funds but limit coverage to specific groups, such as lawfully present immigrants who are in the five-year waiting period for Medicaid coverage, or provide more limited benefits.
Six states, including DC, have recently eliminated or reduced or plan to scale back state-funded coverage due to budget pressures.
- California previously extended state-funded coverage to all income-eligible adults regardless of immigration status but implemented coverage reductions for adults 19 and older who are not pregnant or former foster youth under age 26 due to funding constraints, including: closing enrollment starting January 2026, ending dental benefits starting July 2026, and charging $30 monthly premiums for adults ages 19-59 starting July 2027. The California governor’s 2026-27 budget also proposes applying Medicaid policy changes included in the 2025 reconciliation law (work requirements and more frequent six-month renewals) to adults enrolled in the state-funded coverage program.
- Colorado allows adults regardless of immigration status to obtain Marketplace coverage through OmniSalud using a section 1332 waiver. Colorado uses state funds to provide plans with $0 premiums through SilverEnhanced Savings. The states reduced the enrollment cap for the program from 12,000 in 2025 to 6,700 people due to funding constraints. As noted above, the state also plans to cap enrollment and limit benefits for children and pregnant people beginning in January 2027 due to funding constraints.
- DC provides health coverage to low-income adults 21 and older regardless of immigration status through its longstanding locally funded Healthcare Alliance program. However, DC closed enrollment to adults ages 26 and older and reduced income limits for adults 21 and older starting October 2025. DC plans to end coverage for all adults ages 21 and older by October 2027.
- Illinois extended state-funded coverage to low-income individuals ages 65 and older regardless of immigration status through its Health Benefits for Immigrant Seniors (HBIS) program in December 2020 but new enrollment has been paused since 2023. Illinois previously extended coverage to low-income immigrants ages 42 to 64 regardless of immigration status through the Health Benefits for Immigrant Adults (HBIA) program in 2022, but ended HBIA coverage on July 2025 due to funding constraints.
- Minnesota extended state-funded health coverage to income-eligible adults 18 and older regardless of immigration status in January 2025 but ended this coverage starting January 2026 due to funding constraints.
- Washington uses state funds to provide Marketplace coverage with premium subsidies to individuals with incomes up to 250% FPL regardless of immigration status through Cascade Care using a section 1332 waiver, but funding is limited. In July 2024, Washington extended state-funded health coverage to individuals with incomes up to 138% FPL regardless of immigration status, but the state closed enrollment due to funding constraints and proposes to move current and future enrollees to a limited benefit health care program.
In addition to these states, Maryland also delayed plans to allow income-eligible individuals to purchase Marketplace coverage without subsidies regardless of immigration status to 2028 due to changes in the 2025 reconciliation law that will require additional administrative resources to implement.
Two states (New Mexico and New York) are planning to provide fully state-funded coverage to lawfully present immigrants that will lose Medicaid and ACA Marketplace coverage due to eligibility restrictions in the 2025 reconciliation law. New Mexico plans to use state funds to cover lawfully present immigrants losing Medicaid and ACA Marketplace Coverage in addition to DACA recipients. The New York governor’s 2026-27 budget proposes using state funds to cover lawfully present immigrants losing Medicaid coverage. The state will also use state funds to cover income-eligible lawfully present immigrants losing federally-subsidized health coverage through the Essential Plan. Under a longstanding court ruling, New York is required to provide state-funded coverage to lawfully present immigrants who would be eligible for Medicaid if not for their immigration status. Legislation introduced in New York and several other states, including California, Illinois, and Washington, would expand state-funded health coverage for immigrants to help fill gaps created by the reconciliation law; however, it is uncertain these bills will be enacted.
Impact of State Coverage Expansions on Health Care Access and Use
While coverage expansions for immigrants increase spending, research suggests that they reduce uninsured rates, increase health care use, and improve health outcomes. Data from the KFF/New York Times 2025 Survey of Immigrants show that immigrant adults who live in states that provide more expansive coverage, including the ACA Medicaid expansion for low-income adults overall and immigrant coverage expansions, are about half as likely to be uninsured compared with those living in states with less expansive policies (11% vs. 23%). Other research shows that coverage expansions for immigrant children increase access to health care and are associated with improved health outcomes. A study found that eliminating the five-year wait for Medicaid or CHIP was associated with a decline in uninsured rates among lawfully present foreign-born children in states without state-funded health care programs. California’s 2016 expansion to low-income children regardless of immigration status was associated with a 34% decline in uninsurance rates, and the state’s expansion to all adults was associated with an increase in health coverage among immigrant adults ages 50 and older. Similarly, a study found that children who reside in states that have expanded coverage to all children regardless of immigration status were less likely to be uninsured, to forgo medical or dental care, and to go without a preventive health visit than children residing in states that have not expanded coverage. Another study found that immigrant children residing in states with more expansive health coverage policies were more likely to have uninterrupted health coverage and a usual source of primary care than those residing in states with less expansive health coverage policies. Research has also found that expanding Medicaid coverage to pregnant people regardless of immigration status is associated with higher rates of prenatal care and improved birth outcomes, while more restrictive state coverage policies were associated with reduced postpartum care utilization.
Publisher: Source link