Medicaid is a major source of financing for mental health and substance use disorder care. It covers nearly one-third of all adults with mental illness and nearly one-quarter of adults with substance use disorders (SUD), including many people with more intensive behavioral health needs. This includes adults with serious mental illness (SMI) and nearly half of all adults with opioid use disorder (OUD). Because Medicaid covers a large share of people with behavioral health conditions and finances a substantial share of treatment services and medications, it plays a central role in access to behavioral health care.
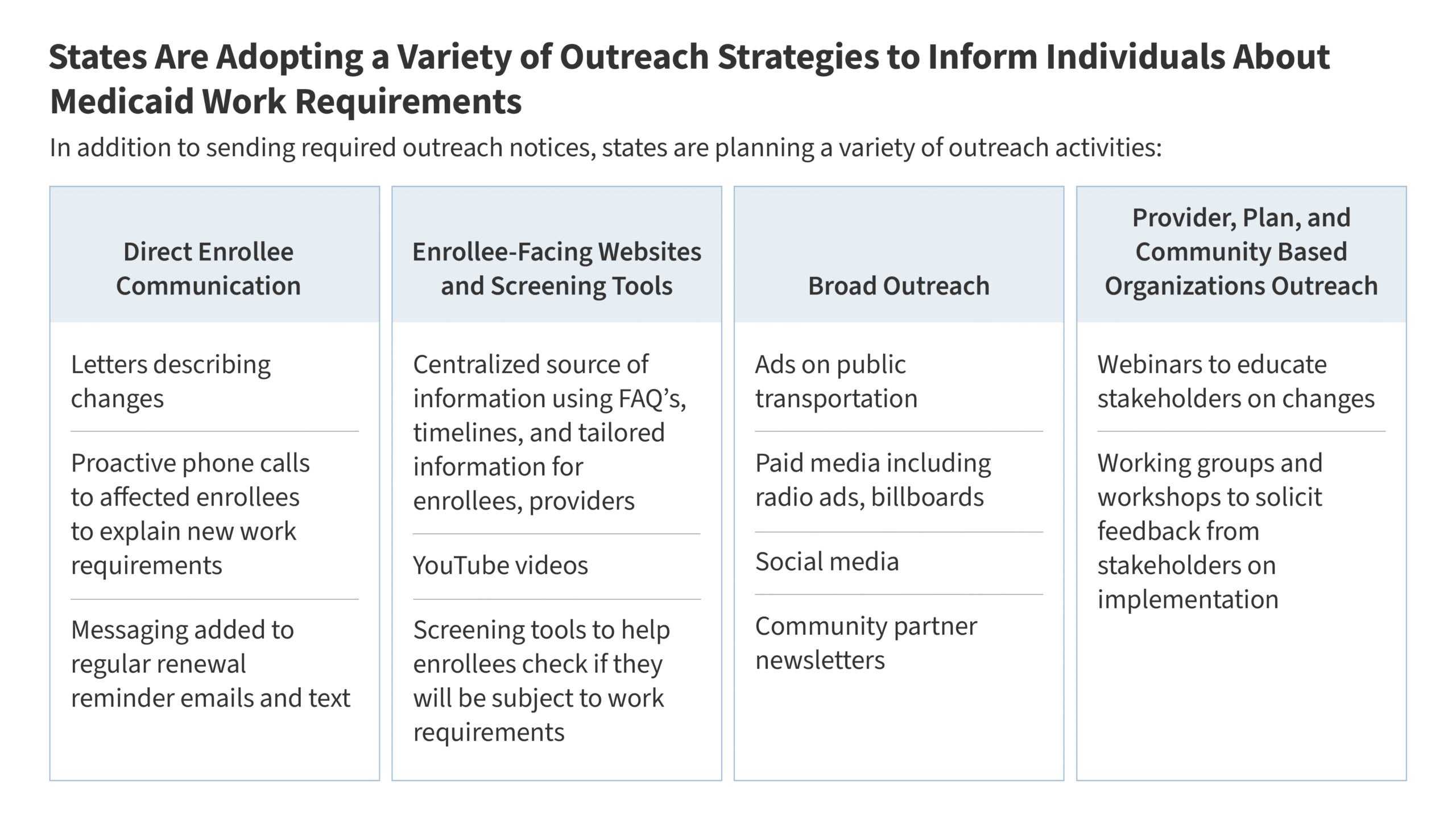
In recent years, many states have used Medicaid to expand the behavioral health treatment continuum and improve access to care. While increasing spending, these changes have helped address longstanding gaps in access to community-based treatment as well as higher levels of care. Benefit expansions have also helped to support state efforts to respond to the opioid epidemic and to build out the behavioral health crisis continuum of care. However, recent federal policy changes, including financing and coverage changes in the 2025 reconciliation law and a more tenuous fiscal climate for states may make those gains harder to sustain. The reconciliation law requires states to implement work requirements (at application and renewal) for Medicaid expansion adults, which is the primary coverage pathway for people with mental health or substance use disorders. These requirements are expected to result in coverage losses, which may interrupt treatment and medication access.
Against this backdrop, this brief examines recent state trends in Medicaid behavioral health coverage and payment and state coverage of select treatment models for people with serious mental illness—a population that has historically faced significant barriers to care. The brief draws on the annual Medicaid budget surveys, conducted by KFF and Health Management Associates (HMA). The 2025 survey included additional detail about coverage of Certified Community Behavioral Health Clinics (CCBHCs) (as a provider type), Assertive Community Treatment (ACT), and Coordinated Specialty Care for First Episode Psychosis (CSC-FEP).
How do recent Medicaid trends reflect state efforts to address mental health and substance use needs?
Behavioral health services are not a specifically defined category of Medicaid benefits. Some fall under mandatory Medicaid benefit categories, such as physician services, while others fall under optional benefit categories, such as rehabilitative services. The ability to cover optional benefits and place limits on items and services results in variation across states. State Medicaid benefit design is also shaped by broader fiscal conditions and federal policy changes.
State efforts to expand Medicaid behavioral health benefits reflect both state priorities and federal opportunities. Since the pandemic and intensifying opioid crisis, behavioral health has become a top priority for many state Medicaid programs. States have focused on expanding access (including in schools), integrating care, and addressing social determinants of health. Federal opportunities, including the SUPPORT Act and American Rescue Plan Act (ARPA), have driven expansions in SUD treatment and crisis services. States have also taken steps to promote more coordinated and integrated care, including adding coverage for services provided under the Collaborative Care Model (CoCM) and enrolling provider types such as CCBHCs that offer a broad continuum of behavioral health services in one setting. Some of these initiatives are part of broader behavioral health state transformation efforts.
Behavioral health has been the most frequently cited category of Medicaid benefit expansion in KFF’s annual budget survey over the past decade. Annually, KFF’s Medicaid budget survey asks state Medicaid officials about recently implemented or planned benefit changes (i.e., benefit enhancements or additions and restrictions or eliminations). In every survey over the past 10 years, behavioral health services were the most frequently reported area of benefit expansions. States reported expansions across the full care continuum of behavioral health services, including institutional, residential, outpatient, home and community-based, peer supports, and crisis services. These trends show how states have used Medicaid to help address longstanding gaps in care and respond to emerging mental health and substance use needs; however future trends are less clear. For example, California’s FY 2026-27 proposed budget would make mobile crisis services optional for counties, rather than statewide and counties that continue to offer the service would have to finance the full non-federal share of costs.
States have also raised fee-for-service (FFS) provider payment rates to help strengthen access to behavioral health services. Even when states add benefits, access may still be limited by provider shortages and narrow networks. Increasing provider rates is one way states have tried to address Medicaid workforce shortages, though rate increases also often face fiscal headwinds. KFF’s Medicaid budget survey asks state Medicaid officials to report annual FFS rate changes for certain provider types. Beginning in FY 2024, KFF’s Medicaid budget survey asked states to report FFS rate changes specifically for outpatient behavioral health clinicians (e.g., psychiatrists, psychologists, clinical social workers, mental health counselors, and marriage and family therapists). More than half of states reported implementing FFS rate increases for one or more outpatient behavioral health providers in FY 2024 and about half of states in FY 2025. The two previous surveys, which asked more broadly about FFS rate increases for any behavioral health provider, found similar numbers of states planning to increase behavioral health provider rates in FYs 2022 and 2023. The size and scope of the rate increases varied, with some states targeting specific provider types or services, while others implemented broader increases. Although most Medicaid enrollees are now in managed care plans, state-set FFS rates often serve as a benchmark or floor for managed care payments in many states. The FY 2025 KFF survey suggests that behavioral health rate increases may be slowing, consistent with reimbursement rate trends for other provider types. About one quarter of states reported plans to increase outpatient behavioral provider rates in FY 2026. This slowdown may reflect the end of pandemic-era federal funds and anticipated federal funding reductions under the 2025 reconciliation law.
What does the FY 2025 KFF budget survey show about selected behavioral health provider types and treatment models?
The FY 2025 annual budget survey asked about state coverage of select optional behavioral health services and provider types: CCBHCs, which provide a broad array of coordinated services in a single setting, and two specialized treatment models for people with SMI: Assertive Community Treatment (ACT) and Coordinated Specialty Care for First Episode Psychosis (CSC-FEP).
State Medicaid recognition of Certified Community Behavioral Health Clinics (CCBHCs) as a provider type continues to grow. CCBHCs are a federally defined model of comprehensive community-based behavioral health clinics that provide or coordinate a core set of mental health and substance use services and serve patients regardless of an ability to pay. In FY 2025, KFF’s Medicaid budget survey asked state officials whether they recognized CCBHCs as a specific enrolled provider type for Medicaid reimbursement in FY 2025 or planned to add the recognition in FY 2026. Nineteen states reported recognizing CCBHCs as an enrolled provider type (Figure 1), up from nine in FY 2022, and several other states reported plans to add CCBHCs as a provider type in FY 2026. This growth has occurred alongside expanded federal support for the Section 223 CCBHC Medicaid demonstration, which gives participating states a pathway to certify CCBHCs, use prospective payments, and receive enhanced federal match rates. States may also add CCBHCs as a provider type through other pathways, including Section 1115 demonstration waivers and Medicaid state plan authority, a state option made permanent through the 2024 Consolidated Appropriations Act. Recognizing CCBHCs as a distinct Medicaid provider type can support more flexible payment approaches, certification of CCBHCs against federal defined criteria, and make CCBHC services easier to identify in claims data. However, formal recognition can require additional state administrative capacity, coordination across state agencies, and operational and budgetary changes. Some states may instead cover behavioral health services provided by CCBHCs through existing provider categories, while others may already have community mental health systems with state-defined service arrays that serve a similar function. Research suggests that CCBHCs have improved access to outpatient behavioral health care, with some evidence of reductions in acute behavioral health care use, such as emergency departments or hospitalization. More than 500 CCBHCs now operate across 46 states, DC, and Puerto Rico.
In FY 2025, two-thirds of states reported FFS coverage for Assertive Community Treatment (ACT), an evidence-based model for people with serious mental illness who need intensive support to remain stable in the community. ACT uses small, multidisciplinary teams to provide 24-hour individualized support in the community and can intensify support when symptoms worsen. It is designed for people with the most serious needs, including those whose severe symptoms and lack of illness awareness can make it difficult to stay engaged in treatment and have higher risk of repeated hospitalization and other disruptions to stable community living. Research suggests that ACT can reduce hospitalizations and improve engagement in care, especially for people with the highest needs and when services are implemented with fidelity to the ACT model. The American Psychiatric Association (APA) guidelines recommend ACT for patients with schizophrenia who have a history of poor engagement with services leading to frequent relapse or social disruption. In KFF’s FY 2025 Medicaid budget survey, 34 states including D.C. reported that ACT is covered under FFS Medicaid for adults (Figure 2). Even in states that report Medicaid coverage for ACT, workforce and infrastructure constraints may limit access. For example, only about one-quarter (27%) of mental health facilities serving people with SMI reported offering ACT services in 2023. Budget pressures may also affect the availability of these services. In Idaho, 2025 budget cuts interrupted ACT services for people who relied on ACT to stay stable in the community, and media reporting documented that some Medicaid enrollees receiving ACT services died after the disruption. Idaho later restored funding, though rebuilding these services may be difficult and costly.
Far fewer states reported FFS coverage for Coordinated Specialty Care for First Episode Psychosis (CSC-FEP), an evidence-based early intervention model for people experiencing a first episode of psychosis. KFF’s FY 2025 Medicaid budget survey asked state officials whether they provide FFS reimbursement for CSC-FEP codes in FY 2025 or plan to do so in FY 2026. Seven states reported covering this service in FY 2025 (Figure 2) and several more states reported plans to add coverage in FY 2026. CSC-FEP emerged in the late 2000s as an early intervention model designed to connect people experiencing psychosis for the first time to coordinated treatment to reduce the serious and potentially lasting effects of untreated psychosis. This model includes coordinated medication management, therapy, family support and education, and other services. Research shows that people who receive this treatment experience fewer psychotic symptoms, fewer preventable hospitalizations, and better outcomes in work, school, and quality of life. The APA guidelines recommend CSC-FEP for patients with schizophrenia experiencing a first episode of psychosis. In addition to the seven states reporting coverage for this model in FY 2025, four more states reported plans to add coverage for CSC-FEP in FY2026, and Virginia reported that coverage approved by its General Assembly will begin in FY 2027. Some states reported that these services are funded outside of Medicaid through the federal Community Mental Health Services Block Grant, which requires states to set- aside 10% of funds for evidence-based programs for people with early serious mental illness.
This work was supported in part by the Philos Foundation. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Publisher: Source link