Introduction
On March 1, 2025, President Trump signed Executive Order (EO) 14224 designating English as the official language of the United States. This marks the first time in the country’s history that the U.S. has declared an official language at the federal level. Although the Order does not by itself trigger changes in services provided by agencies or organizations receiving federal funding, the policy represents a departure from previous administrations’ policies around language access for individuals with limited English proficiency (LEP). The federal government defines people with LEP as those who do not speak English as their primary language and who have a limited ability to read, write, speak, or understand English (also described as speaking English “less than very well”).
An accompanying official fact sheet released by the Trump administration outlines how EO 14224 will affect agencies and their services, including review of all services currently offered in languages other than English and phasing out of non-essential services. Prior guidance for agencies serving people with LEP has been suspended.
The Order will likely result in more limited availability of language access services for people with LEP. Language and interpretation services are important for ensuring access to health coverage, care, and for improving health outcomes. Loss of services may further exacerbate disparities in health and health care, as people with LEP are disproportionately more likely to be Hispanic, Asian, immigrants, and to have lower incomes. Further, the new EO could also create challenges and confusion for health care and other service providers, who remain subject to other laws and regulations that still require provision of language access services.
This issue brief provides an overview of EO 14224 and its potential implications for multilingual resources, including data on the shares of individuals with LEP across different socioeconomic characteristics based on KFF analysis of 2023 American Community Survey (ACS) data.
Prior Language Access Policies
Prior laws and guidance have established requirements for language access and protection for people with LEP. Title VI of the Civil Rights Act of 1964 and Section 1557 of the Affordable Care Act (ACA) prohibit discrimination based on national origin, including discrimination based on the ability to speak English. Previously, the Department of Justice (DOJ) took the stance that Title VI of the Civil Rights Act prohibited discrimination against people with LEP, recognizing that a lack of language access represented discrimination based on national origin. In 2000, President Clinton issued EO 13166, which required all federal agencies to ensure meaningful access to services for people with LEP and established that failing to provide adequate services would be considered discrimination based on national origin. EO 14224, signed by President Trump, revokes EO 13166 and any policy guidance documents issued under it, and requires the Attorney General to provide updated guidance.
Section 1557 of the Affordable Care Act strengthened language access protections by prohibiting discrimination in health programs and other services that receive federal financial assistance. Section 1557 requires covered entities, including hospitals, clinics, insurers, and state Medicaid programs, to provide meaningful access for individuals with LEP. While Section 1557’s protections took effect when the ACA was enacted in 2010, much of its reach has been determined by implementation guidance issued across different presidential administrations. Under the Biden administration regulations issued in 2024, entities that operate health programs or activities and receive federal financial assistance must take reasonable steps to provide meaningful access to individuals with LEP who are eligible to be served or likely to be directly affected by the program or activity. The regulation specifies requirements regarding how the services must be provided, including that they be free of charge, accurate, and timely; outlines standards for interpretation and translation services; and identifies requirements for entities to provide notice of the availability of services. Section 1557 remains in effect despite the Executive Order, meaning that health care entities will continue to be required to provide language access services, even as federal agencies may scale back their language access resources.
Changes in Language Access Under the Trump Administration
EO 14224, issued by President Trump in March 2025, declares English as the official language of the U.S. and revokes prior orders requiring federal agencies to provide meaningful access to services for individuals with LEP. The Order also instructs the Attorney General to rescind all policy guidance stemming from EO 13166. As a result, in April 2025, the DOJ rescinded its 2022 LEP guidance, which directed agencies to assess and enhance their language access policies, and published a new memorandum providing implementation guidance related to the EO. The DOJ also removed LEP.gov, a website that provided resources to federal agencies and other entities receiving federal funding for developing language access plans.
Patients are still entitled to interpreter services under Title VI through qualified bilingual staff or interpreter services at no additional cost. Historically, providers have often aligned their services with the Department of Health and Human Services (HSS) outlined National Standards for Culturally Linguistically Appropriate Services (CLAS), a set of 15 voluntary guidelines designed to advance language access and cultural competence in healthcare. These standards include informing individuals of language assistance availability, ensuring the competence of individuals providing translation services, and providing written translation of key documents such as health consent and education documents. While the CLAS standards are not a binding federal regulation and therefore cannot be revoked by EO 14224, their adoption and implementation may decline as changes to federal language access policies reduce oversight, investment, and incentives for compliance.
The new memorandum recommends that federal agencies scale back the provision of language services, minimizing non-essential multilingual services, and recommends that agencies consider offering services exclusively in English. However, it does not require agency heads to amend, remove, or otherwise stop the production of documents, products, or other services prepared or offered in languages other than English. Despite these ongoing requirements, the new guidance signals that the DOJ will no longer treat a lack of multilingual services as discrimination, and that agencies are no longer required to implement wide-scale language access plans.
The EO and accompanying DOJ guidance apply only to federal government agencies and do not change existing language access requirements under laws like Title VI of the Civil Rights Act or Section 1557 of the ACA. Executive Orders cannot overturn existing statutes and regulations that go through formal revisions and public notice and comment processes. Title VI and Section 1557, which were issued by HHS, outline compliance measures that cannot unilaterally be changed by Executive Order. Entities that receive federal funding including state and local health departments, hospitals, insurance companies, clinics, and other health care providers remain legally obligated to provide meaningful language access under these laws. Under Section 1557 regulations, forms such as informed consent documents, intake forms, and discharge instructions are still required to be translated for individuals with LEP. Moreover, several states, including, New York, California, Hawaii, Maryland, and the District of Columbia, have state-level language access laws that remain in effect. However, the reduction in federal oversight, and granting agencies the ability to decide how and when to offer services in languages other than English, including at HHS and the DOJ, may create uncertainty about implementation and compliance practices, and reduce the availability of federal resources for providing language access services. Enforcement is also likely to shift since the DOJ has narrowed its interpretation of Title VI, indicating that it will no longer pursue enforcement based on disparate impact claims related to language access, instead, it will now focus on cases involving intentional discrimination. This change in enforcement could impact accountability measures and ultimately weaken protections for individuals with LEP.
Who is Likely to Be Affected by Reductions in Language Access Services?
Over 27 million people in the U.S. have LEP and may be affected by decreased access to language access services, with disproportionate impacts on Asian and Hispanic people, immigrants, and people with lower incomes. Data from the 2023 ACS show that 9% of the population ages 5 and older, or 27.3 million individuals, have LEP (defined as speaking a language other than English at home and speaking English less than very well). Asian (30%) and Hispanic people (29%), immigrants (47%), and those with incomes under $40,000 per year (13%) are disproportionately more likely to have LEP than the overall population (Figure 1). Decreased access to language assistance services comes at a time when immigrants are facing other barriers to accessing health care and other services, including increased immigration-related fears and more limited eligibility for health care coverage and other services.
Decreased access to language assistance services would have greater effects in some states, since there are wide variations in the shares of people with LEP across states (Figure 2). The share of people ages 5 and older with LEP ranges from less than 1% in West Virginia to 18% in California. New York (14%), New Jersey (14%), Texas (13%), and Florida (13%) also have relatively high shares of individuals with LEP, likely reflecting larger numbers of immigrants residing in those states.
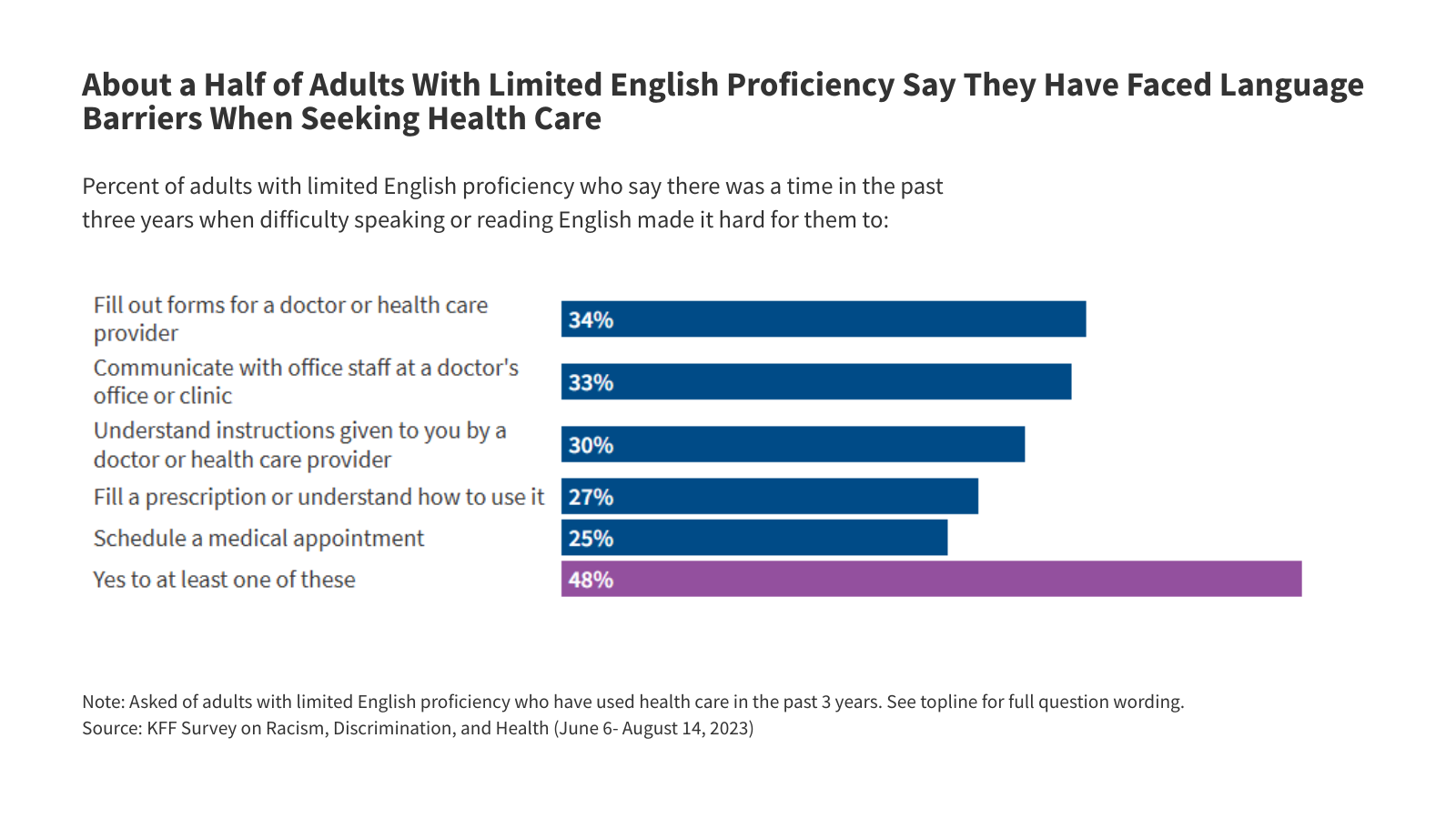
Language access services have important implications for health and health care. People with LEP face challenges and barriers to accessing high-quality health care. Language barriers between providers and patients can reduce the quality of care and increase the risk of adverse outcomes or medical errors. Studies have found that a lack of language assistance often delays patients’ access to timely care, leading to poor chronic disease management and resulting in worse health outcomes. Despite existing language access requirements, KFF survey data find that around half (48%) of adults with LEP have encountered at least one language barrier in a health care setting within the past three years, such as difficulty filling out forms for a health care provider (34%), communicating with office staff at a doctor’s office or clinic (33%), understanding instructions given by a doctor or health care provider (30%), filling a prescription or understanding how to use it (27%), or scheduling a medical appointment (25%) (Figure 3). Among adults with LEP, one in five reported experiencing at least one of several negative experiences with a health care provider in the past three years, including a provider ignoring a direct request or question (11%), assuming something about them without asking (8%), suggesting they were personally to blame for a health problem (8%), or refusing to prescribe needed pain medication they thought they needed (8%).
Reductions in requirements for federal agencies to provide language access services may create new challenges for health care and other service providers. If federal agencies reduce language access guidance and requirements, providers will have fewer translated materials to rely on, such as consent documents and health education materials. This can also create inconsistencies in the quality and accuracy of materials across the health care landscape. Community health centers (CHCs) and other safety net providers may be disproportionately impacted by the reduced availability of federal language access resources as they are disproportionately likely to serve individuals with LEP and those with lower incomes. Federal cuts have already eliminated funding for community workers who help people who speak other languages navigate and sign up for health insurance coverage. Moreover, given differences between the new guidance and other laws that remain in place, providers may have questions or confusion about when translation services are required, compliance risks, and how comprehensive services must be.
Publisher: Source link